

When discussing rhinoplasty, the prevailing narrative often leans heavily toward aesthetic enhancement. However, a crooked nose represents a complex intersection of facial asymmetry and physiological dysfunction. It is rarely a mere cosmetic concern; rather, it is frequently the visible manifestation of underlying anatomical pathologies that impede respiration. For patients suffering from chronic rhinitis, sleep apnea, and reduced concentration due to hypoxia, a permanent crooked nose fix requires a dual approach: aesthetic realignment combined with functional restoration.
At View Plastic Surgery, we approach the deviated nose correction through the lens of functional rhinoplasty. This discipline goes beyond surface-level straightening to address the skeletal and cartilaginous framework responsible for nasal obstruction. This comprehensive clinical review explores the etiology of the crooked nose, the necessity of concurrent functional repair, and the advanced surgical protocols utilized in rhinoplasty Korea.
Defining the Crooked Nose
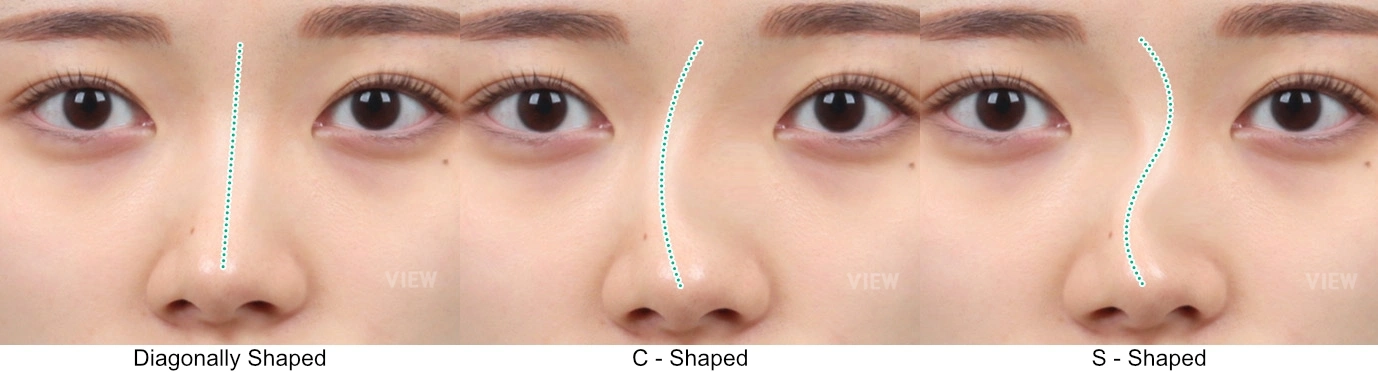
Clinically, a crooked nose is defined as a deviation of the nasal pyramid from the mid-sagittal plane of the face. This deviation involves the osseous (bony) upper third and the cartilaginous lower two-thirds of the nose. While the visual diagnosis is straightforward—manifesting as a C-shape, S-shape, or linear slant—the internal architecture is often far more chaotic. The external deformity is almost invariably accompanied by a deviation of the nasal septum, the vertical wall dividing the nasal cavity.
The etiology of a crooked nose is typically categorized into two primary vectors:
- Congenital/Developmental: Deviations occurring during the growth of the vomer and perpendicular plate of the ethmoid bone, often exacerbated by unequal pressure during childbirth or genetic predisposition.
- Traumatic: Resulting from distinct nasal bone fractures or micro-fractures that healed via malunion. In these cases, the septal cartilage may dislocate from the maxillary crest, creating a physical blockage.
Understanding this distinction is crucial for surgical planning. A traumatic deviation often requires osteotomies (controlled bone breaking) to reset the foundation, whereas developmental deviations may require extensive septal grafting to straighten the structural axis.
The Pathophysiology of Obstruction: The Hidden Costs of a Crooked Nose
The correlation between a crooked nose and nasal disease is not incidental; it is anatomical. The nasal airway functions as a resistor; when the structural geometry is compromised, airflow resistance increases exponentially. This leads to a cascade of physiological issues commonly treated in rhinoplasty procedures focused on function.
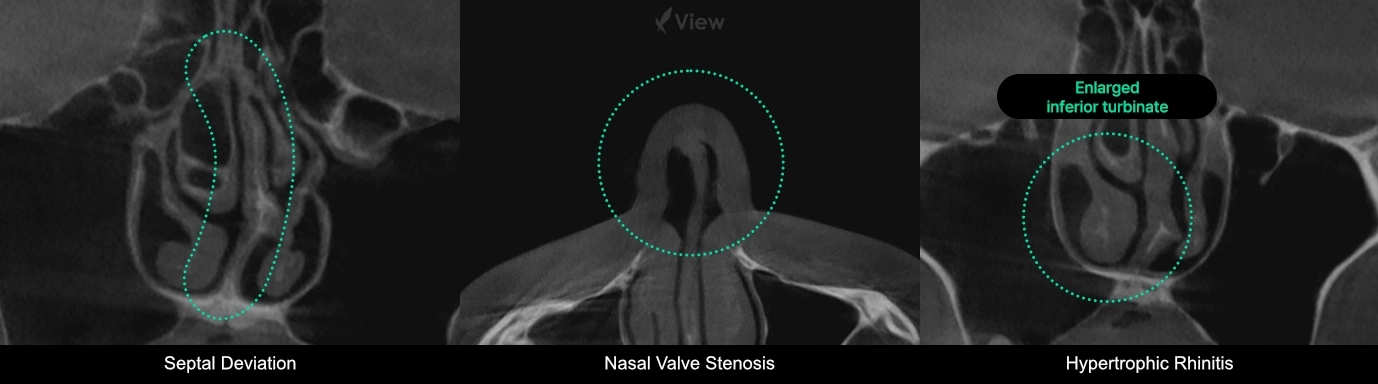
Septal Deviation and Airflow Dynamics
When the septum deviates, it narrows one nasal passage. According to the Bernoulli principle, as air moves faster through the narrowed passage, pressure drops, potentially causing the nasal valve to collapse inward during inspiration. Conversely, the wider side often develops compensatory turbinate hypertrophy—where the turbinate tissue swells to fill the excess space—paradoxically causing obstruction on both sides.
Chronic Rhinitis and Sinusitis
Impaired mucociliary clearance due to structural blockages allows pathogens to linger in the nasal cavity. This creates a chronic inflammatory state, manifesting as perpetual congestion, post-nasal drip, and recurrent sinus infections that do not respond permanently to pharmacotherapy.
Systemic Hypoxia Effects
Chronic nasal obstruction forces mouth breathing, which bypasses the nose’s filtration and humidification functions. This leads to dry mouth, sore throats, and significantly, sleep fragmentation. The resultant lack of deep REM sleep contributes to chronic fatigue, cognitive decline, and reduced concentration—complaints frequently voiced by patients seeking a crooked nose job.
Functional Rhinoplasty: The Surgical Standard
Functional rhinoplasty is the surgical recalibration of the nasal airway. Unlike standard cosmetic rhinoplasty, which may compromise structural integrity to achieve a smaller shape, functional rhinoplasty prioritizes the patency of the airway. This often involves strengthening the nasal valves and straightening the septum while refining the external appearance.
| Component | Aesthetic Goal | Functional/Medical Goal |
|---|---|---|
| Nasal Septum | Straighten the midline to correct visible nose slant. | Septoplasty: Remove or reshape deviated cartilage to open airways. |
| Nasal Turbinates | N/A (Internal structure) | Turbinoplasty: Reduce hypertrophied tissue using radiofrequency or resection. |
| Nasal Valves | Define the dorsal aesthetic lines. | Spreader Grafts: Widen the internal valve angle to prevent collapse during inspiration. |
| Nasal Bones | Narrow the bridge width; remove humps. | Osteotomy: Break and reset malunited bones to restore symmetry. |
Diagnostic Precision: The Pre-Operative Protocol
A successful outcome relies heavily on accurate diagnosis. At View Plastic Surgery, we employ a rigorous diagnostic protocol that integrates plastic surgery aesthetics with otorhinolaryngology (ENT) functionality.
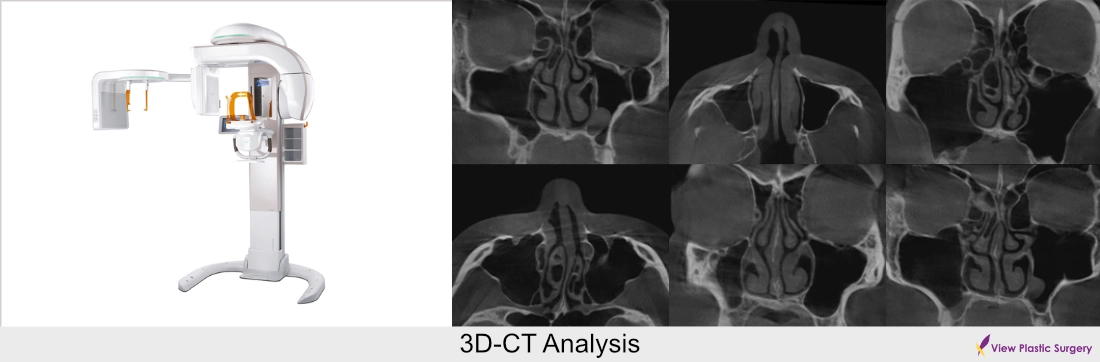
1. 3D-CT Analysis: Two-dimensional X-rays are insufficient for nasal surgery. We utilize high-resolution 3D-CT scanning to visualize the septal cartilage, bone structure, and turbinate hypertrophy in three dimensions. This allows for the precise mapping of the septal deviation—whether it is caudal, dorsal, or deep within the vomer.
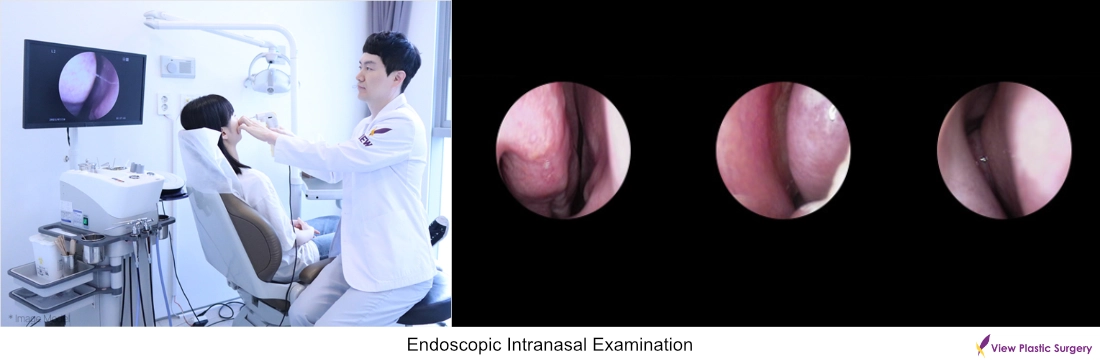
2. Endoscopic Intranasal Examination: To assess the health of the mucosa and identify polyps or chronic sinusitis, a fiber-optic endoscope is used. This step is critical to ensure that any soft tissue pathology is addressed concurrently with the skeletal reconstruction.

3. Collaborative Approach: We emphasize a multidisciplinary approach where plastic surgeons and ENT specialists collaborate. This ensures that while the plastic surgeon focuses on the aesthetic profile and symmetry, the functional aspects are treated with medical rigor.
Surgical Methodology: Correcting the Deviated Framework
The surgical correction of a crooked nose is among the most technically demanding procedures in facial plastic surgery. It requires a tiered approach utilizing various grafts and osteotomies.
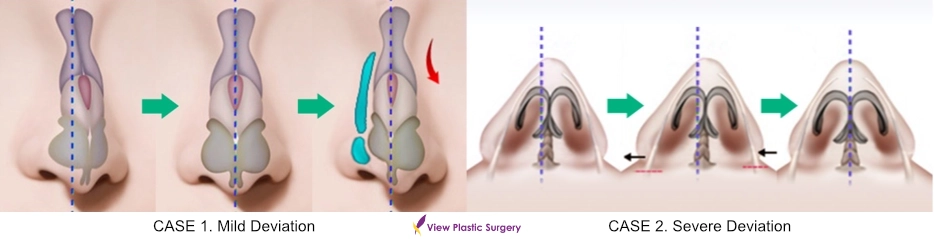
Medial & Lateral Osteotomies
To correct the bony upper third of the nose, controlled fractures (osteotomies) are performed. Lateral osteotomies mobilize the nasal bones, allowing them to be shifted to the midline. In cases of severe asymmetry, intermediate osteotomies may be required to flatten a convex side or elevate a concave side.
Septal Reconstruction and Spreader Grafts
The septum is the pillar of the nose. In a crooked nose fix, the deviated portion of the septum is removed or scored and repositioned (Septoplasty). Crucially, to prevent the nose from reverting to its crooked state (due to cartilage memory), spreader grafts are often employed. These are rectangular strips of cartilage placed between the septum and upper lateral cartilages. They serve two purposes: they act as splints to keep the septum straight, and they widen the internal nasal valve to improve breathing.
Tip Derotation and Symmetry
Often, a crooked nose is accompanied by a tip that is rotated or asymmetrical. Using columellar struts or septal extension grafts, the tip is anchored to the newly straightened septum, ensuring that the external tip projection aligns perfectly with the facial midline.
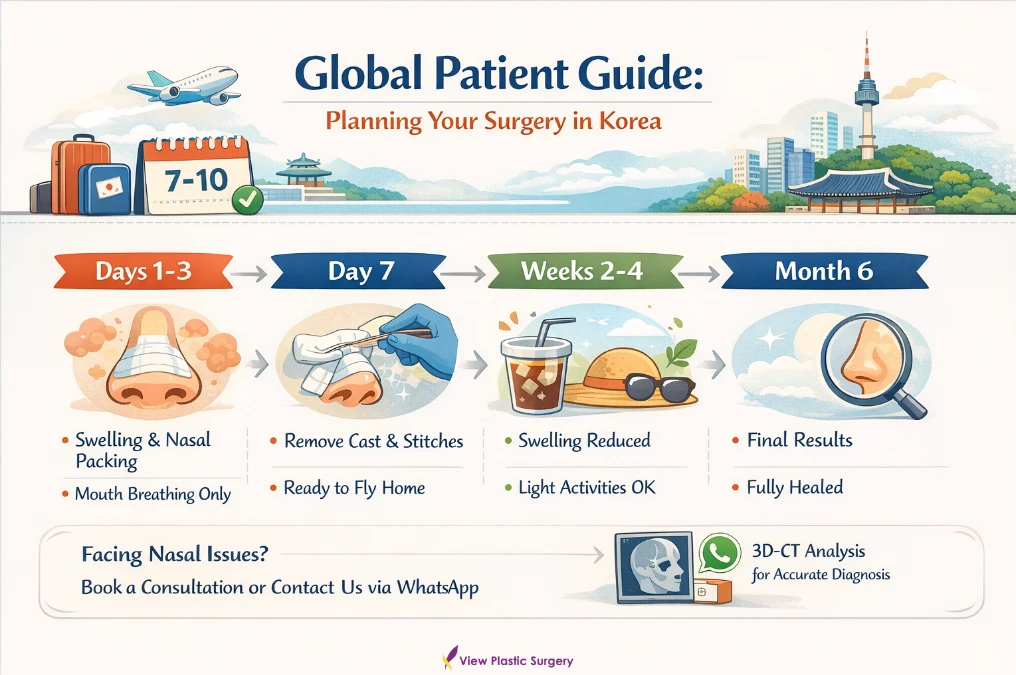
Global Patient Guide: Planning Your Surgery in Korea
For international patients seeking rhinoplasty Korea, logistical planning is as vital as the surgery itself. View Plastic Surgery provides a streamlined pathway for overseas visitors.
Recommended Stay: We recommend a stay of 7 to 10 days in Korea. This window allows for the initial surgery, post-operative observation, and the removal of stitches and nasal splints (casts).
Recovery Timeline:
Day 1-3: Significant swelling and packing in the nose (removed usually on Day 2 or 3). Mouth breathing is required during this phase.
Day 7: Removal of external cast and columellar stitches. Patients can usually fly home after this appointment.
Week 2-4: Major swelling subsides. Return to non-strenuous social activities.
Month 6: Final structural stability and aesthetic refinement.
If you are suffering from the dual burden of facial asymmetry and nasal obstruction, we invite you to book a consultation or contact our team directly via WhatsApp. Accurate diagnosis via 3D-CT is the first step toward a permanent solution.













